- Mar 13
Painful periods: why they happen & how to actually help them.
- Shabina
- Menstrual Cycle
- 0 comments
Cramping so bad you can't get out of bed. Back pain that radiates into your legs. Headaches, nausea, breast tenderness. If this sounds familiar — you're far from alone. But here's the thing: painful periods are common. They are not normal.
Intense uterine cramps, lower back pain, breast tenderness, migraines — a huge number of women live with painful periods every single month. According to INSERM, 90% of menstruating women aged 18–49 experience dysmenorrhoea (the medical term for painful periods). It is the leading cause of school absenteeism in young women.
And yet, far too often, these women are told it's just part of being a woman. That they should take a painkiller and get on with it. This article is for everyone who has ever been dismissed — because painful periods are not inevitable, they are not trivial, and solutions absolutely exist.
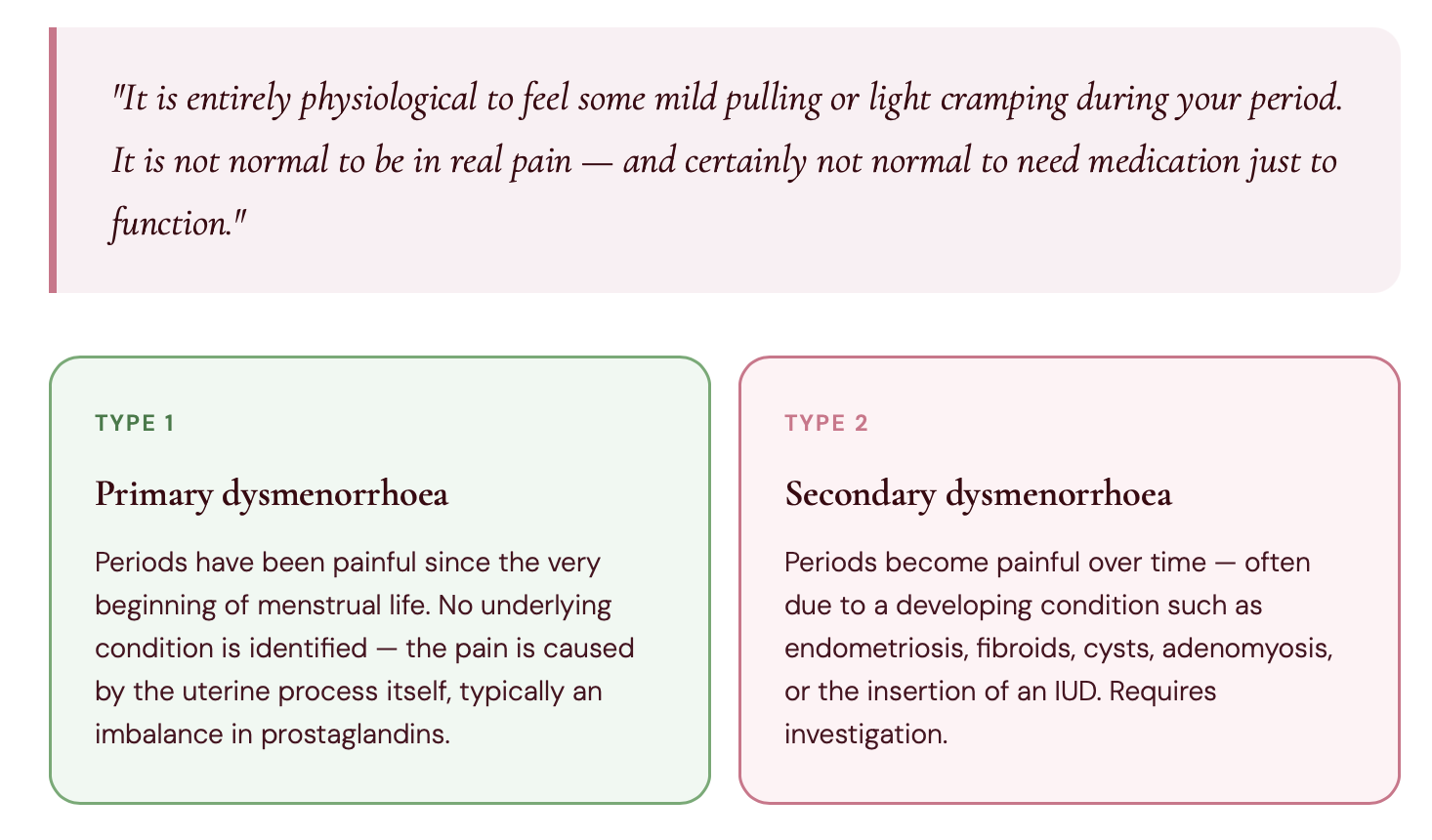
What are painful periods, exactly?
Doctors use the terms dysmenorrhoea or algomenorrhoea to describe painful periods — but the experience is the same: significant pain during menstruation, especially in the first days, which requires medication to be managed. Pain can be concentrated in the lower abdomen, or radiate into the lower back and legs.
In the most severe cases, standard treatments like NSAIDs (non-steroidal anti-inflammatory drugs) don't work at all, and stronger medical interventions are needed.
What actually causes painful periods?
Painful periods can have multiple causes — hormonal, mechanical, inflammatory, or a combination of all three. Crucially, they are not always a sign of endometriosis. Here is a full picture of what can be going on.
The link between painful periods and PMS
PMS (premenstrual syndrome) typically occurs before your period and eases once it begins. But many women find their PMS transitions directly into painful periods — and there's a reason for that.
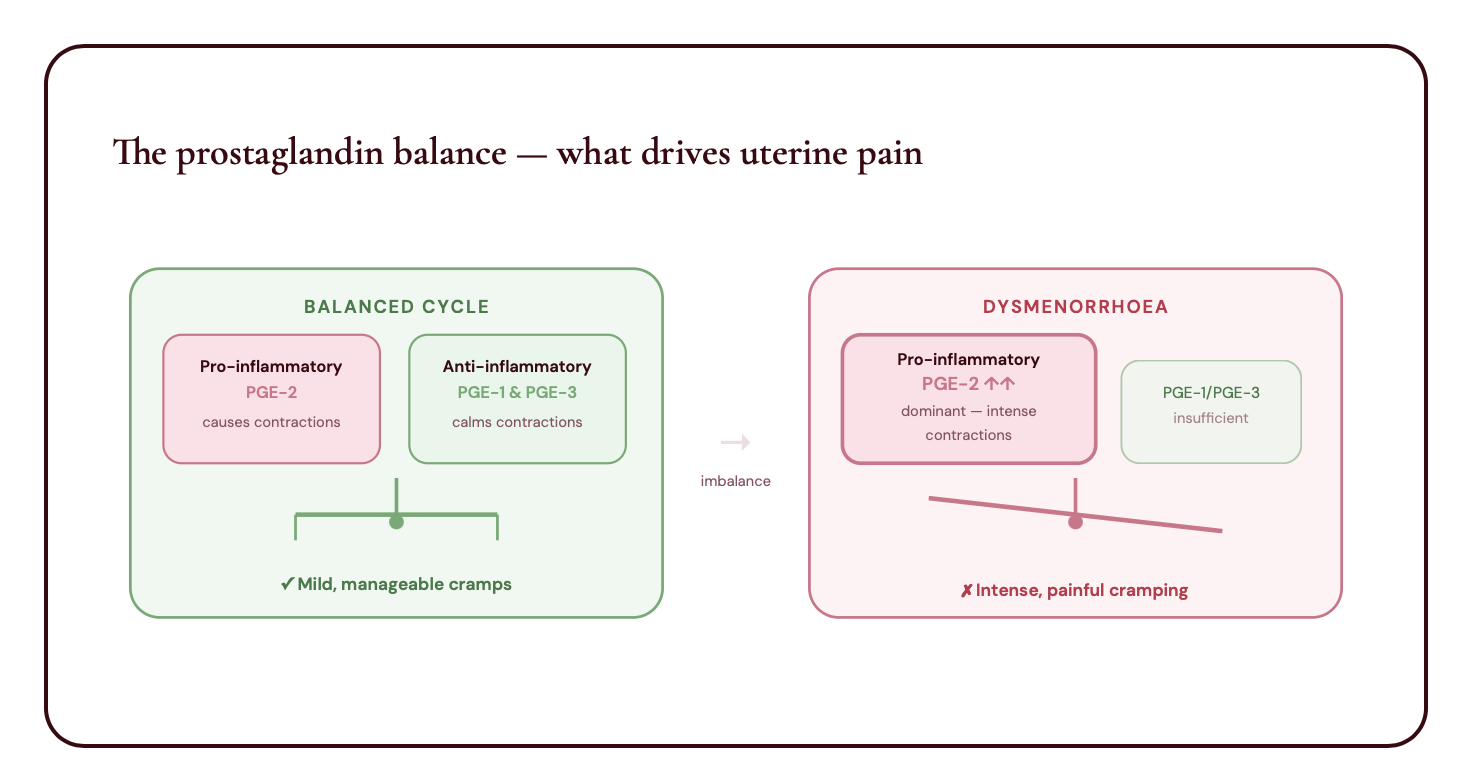
The root causes of both are closely connected: a dominance of pro-inflammatory prostaglandins driving strong uterine contractions, combined with an oestrogen-progesterone imbalance in the second half of the cycle.
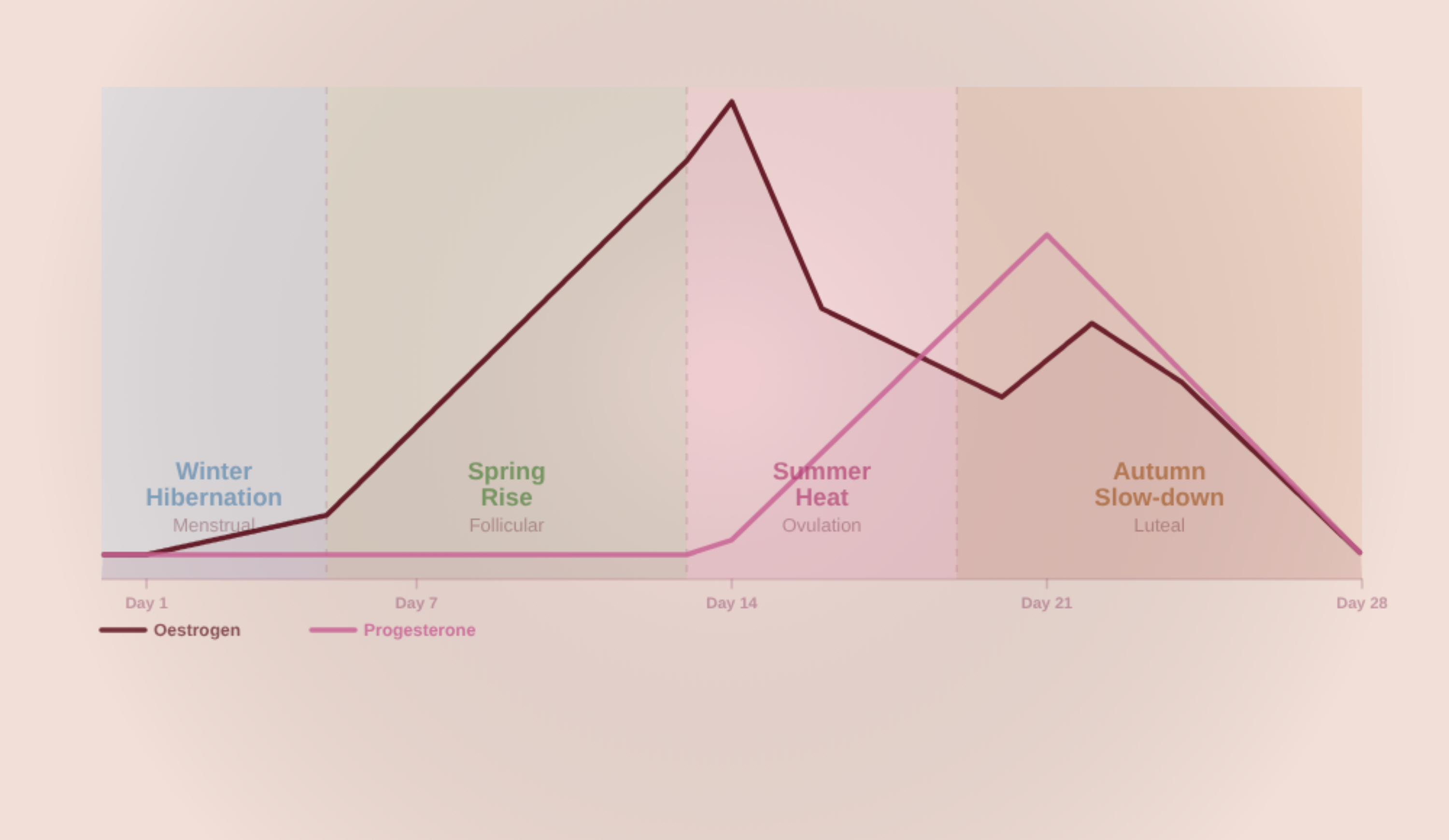
When oestrogen is dominant in the second half of the cycle, it thickens the uterine lining further — meaning the uterus must contract harder to shed it, making periods more painful and more abundant. If progesterone was insufficient during the luteal phase, the lining didn't receive proper blood supply and detaches in larger pieces, intensifying the pain further.
That said, the two are not always linked. Some women have painful periods without PMS(especially when the cause is mechanical — an IUD, cyst, fibrome), and some have PMS without painful periods, finding relief once their period actually begins.
Why painful periods deserve to be taken seriously
Painful periods are rarely dangerous in the acute sense — but dismissing them as "just part of being a woman" is both medically inaccurate and deeply unhelpful. Here's why they matter:
How to actually help painful periods
If you've complained to a doctor about your periods being painful, they probably guided to towards these options :
Medication / paracetamol
The problem with anti-inflammatories is that they can interfere with ovulation, since ovulation requires a mild inflammatory process to rupture the follicle. Worth being aware of if you're tracking your cycle.
HORMONAL CONTRACEPTION
Often prescribed for painful periods. It does not treat the hormonal imbalance — it simply suppresses the cycle. Can be appropriate short-term but does not address root causes.
In other words, medical options are very limited and don't get to the root cause of your pain.
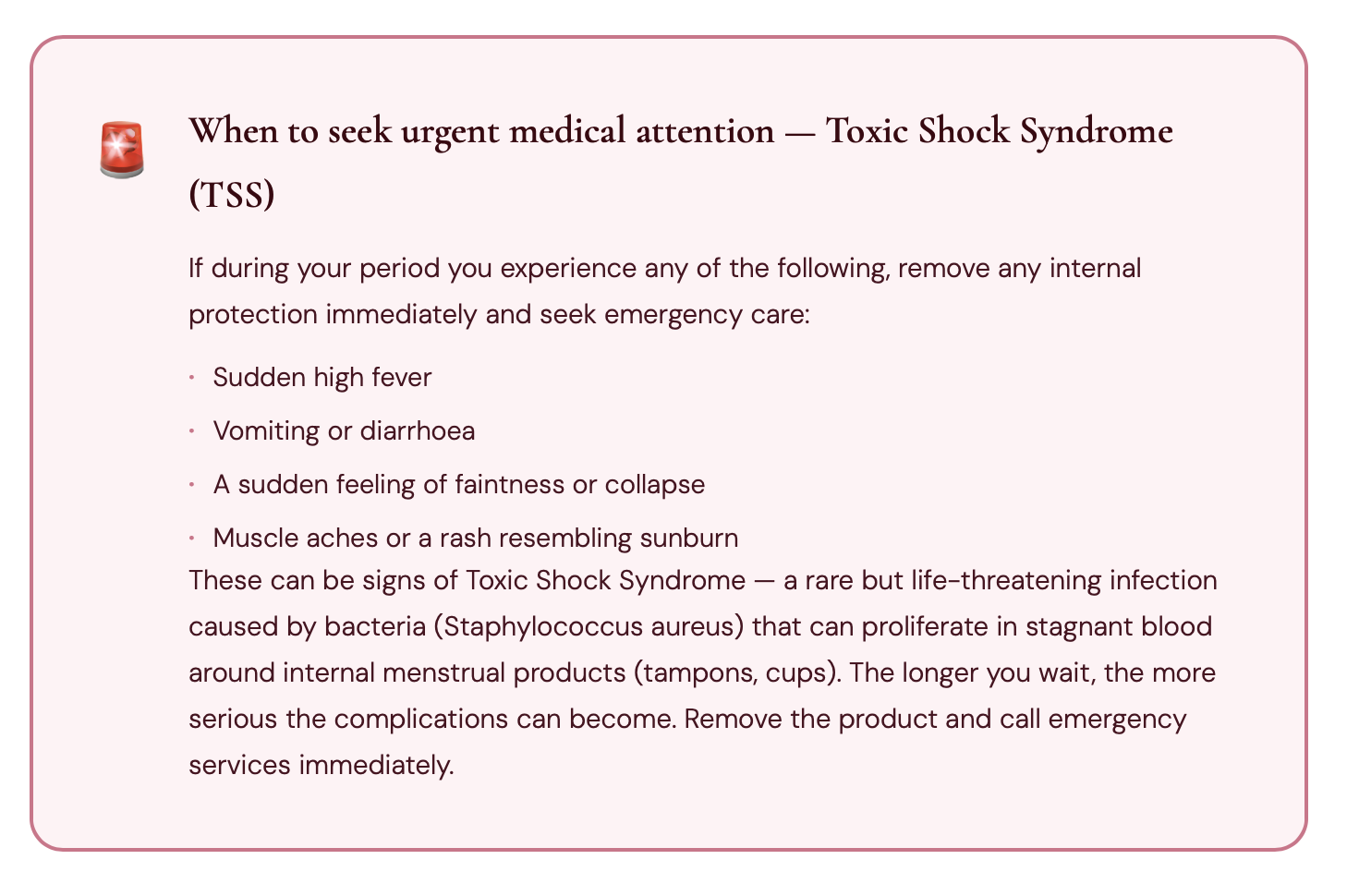
When to see a health practitioner —and when to go urgently
As a general rule: if your period pain requires medication to be manageable, see a health practitioner That threshold alone is your signal.
Your period pain requires medication to function through the day
You've suddenly developed painful periods when they were fine before (secondary dysmenorrhoea)
Your periods are accompanied by very heavy bleeding
You suspect endometriosis — especially if pain extends beyond your uterus
You have an IUD and believe it may be contributing to your pain
Pain is affecting your work, studies, relationships or mental health
Your doctor or gynaecologist can perform an ultrasound to check for fibroids or cysts, run a hormonal panel, investigate endometriosis, or discuss removing an IUD. There is always a next step.
The bottom line
Cramps and period pain that stop you from functioning are not normal — and they are not something you simply have to endure. Whether the pain comes from a hormonal imbalance, an inflammatory load, a mechanical cause, or a condition like endometriosis, there is always a reason, and there is always something that can be done.
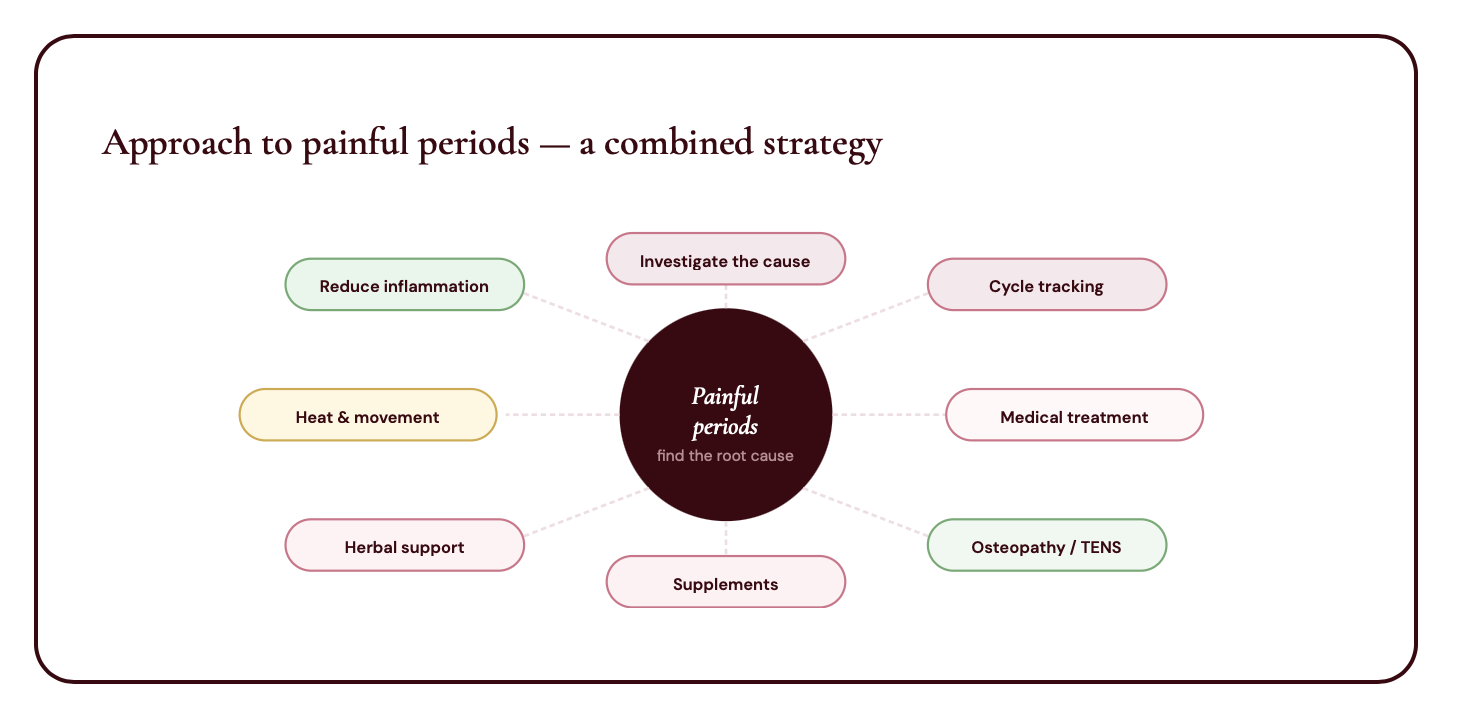
The best approach is usually a combination: a medical investigation to understand the root cause, alongside natural, lifestyle-based strategies that reduce inflammation and support your hormonal balance over time. These two approaches are not in competition — they are complementary.
The same applies to associated pain: lower back tension, breast tenderness, headaches. These symptoms are often dismissed as minor. They are not catastrophic, true — but they are your body's signals, and they deserve to be listened to.